Interesting (but rare) cases rarely come in, when they do, it is the right time to foot the pedal and start learning new things. I was digitally and remotely presented with a case of Prader-Willi Syndrome (PWS). This case was originally presented to a physiotherapist-in-training in Malaysia. I was contacted to give my insight about the syndrome and hell yeah I learned this from one the “hard” classes, Eukaryotic Gene Regulation and Diseases a.k.a gene reg.
First and foremost, note that PWS has a sister syndrome that shares a little bit similarity with regard to the genetic defects. The sister disease is known as Angelman Syndrome (AS). Both diseases happen due to defects in the chromosome 15. Let’s talk about the PWS first and then we compare it with AS.
PWS is unique because it is not the classic case of “oh your parent(s) got mutated copies of genes, therefore, you inherit them”. It is not precisely like that. PWS is a syndrome to which it is concerned with the activation state of some genes on chromosome 15. When we talk about activation state of genes, the genes are there but being silenced. Let’s talk about silencing genes some other time because there are many ways genes can be silenced.
So what happened with PWS, exactly?
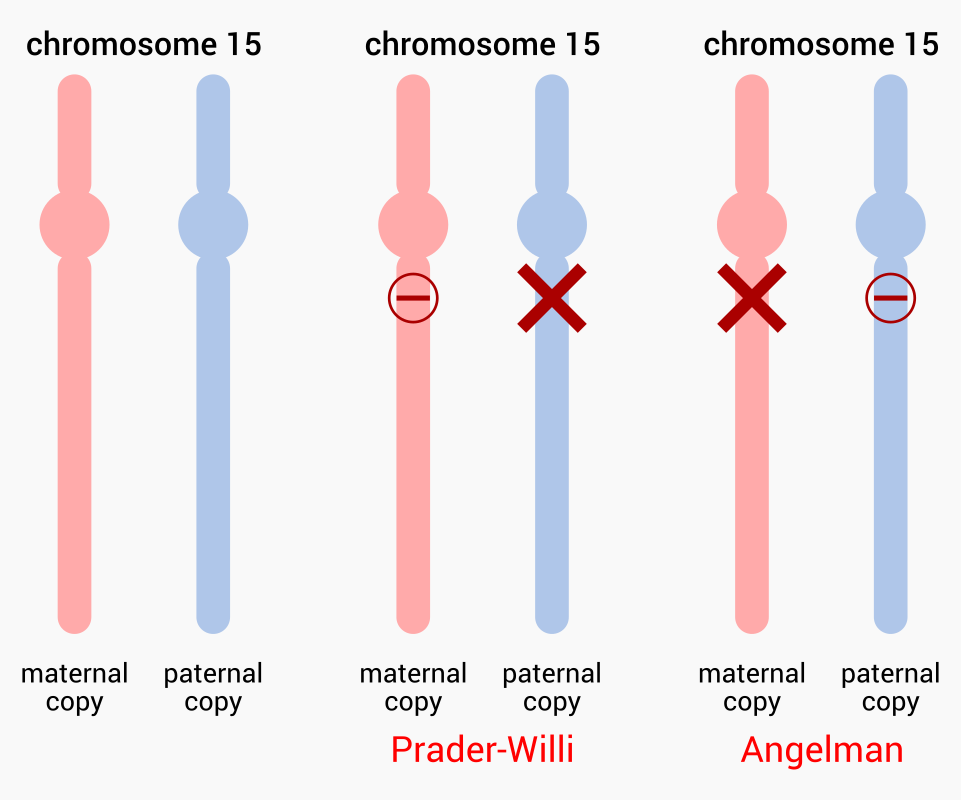
Each person has two copies of the same chromosome right? One from mom, another from dad. For a patient with PWS, a region on the chromosome 15 (15q11-13) from dad—paternal copy—is deleted and people think those genes are, among others, SNRPN and necdin. One would think that since we have mom’s copy of the chromosome 15, it would be sufficient, right?
No.
Enter, genomic imprinting. There are some genes that we inherit from either parent being constitutively inactive. As for PWS, mom’s copy of genes SNRPN and necdin are rendered inactive. To summarize, the paternal copy got deleted and mom can’t compensate. Clinical manifestation: the kid could be too big and short with varying degree of developmental delay
What about AS?
Same idea with a different set of genes but it is the reversed. For a patient with AS, a region on the chromosome 15 (15q11-13) from mom—maternal copy—is deleted and that gene is usually UBE3A. Dad’s copy of the chromosome does not express this gene since it is inactive. To summarize, the maternal copy got deleted and dad can’t compensate. Clinical manifestation: happy puppet syndrome.
Why is gene imprinting important? I don’t know. I would theorize that having two copies of the same genes being active would lead to increase in gene dosage that eventually could make things worse for some cases. I rest my case here.
Update! Let’s briefly discuss the uniparental disomy.
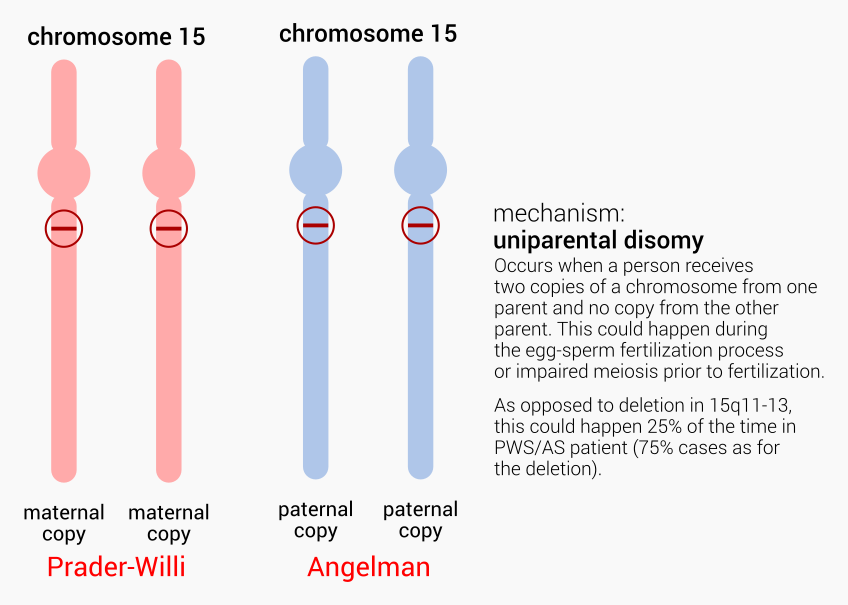
It is possible that a person could receive no chromosome 15 at all from either parent but has two copies of the chromosome 15 from one parent. This is what we call the uniparental disomy, or UPD for short. If a person has two maternal copies of the chromosome 15, that’s Prader-Willi syndrome. If a person has two paternal copies of the chromosome 15, that’s Angelman syndrome.